
Micki Duerre (Principal Clinical Research Associate)
Traceability Starts at the Source: Part 1, Navigating eCRFs, Worksheets, and eSource
Why Missing Source Matters
In my experience as a monitor, the fastest way to uncover hidden risks in a clinical trial is to start with the source. Source documentation tells the story the case report forms (CRFs) cannot.
The importance of complete and verifiable source documentation becomes clear when looking at industry-wide trends. In 2024, data Integrity issues ranked second among the top 10 FDA 483 Observation1. One of the most frequent findings during audits and inspections is data recorded without verifiable source documentation. When data in case report forms cannot be verified against source documents, it raises concerns about:
- Trial conduct and credibility
- Regulatory risk which can lead to findings during audits or inspections, and could confound trial results
- Safety and risks to participants and future patients, including potential product mislabeling
Understanding these risks sets the stage for why strong collaboration between the sponsor/Contract Research Organization (CRO) and the clinical site is essential. Behind every successful clinical trial is the partnership of these teams. It is the job of the clinical site to enroll participants, collect data, and capture all observations, findings, and activities necessary to reconstruct the conduct of the clinical study at the site. It is the job of the sponsor and/or CRO to have qualified monitors review the source documentation, document the type and location of source records, and ensure every data point is traceable from data collection to data entry.
The following discussion is the first of a three-part series covering the fundamentals of source documentation, electronic source documentation and certified copies, and methods of documenting the type and location of source records.
1Top 10 FDA 483 Observations of 2024—and How to Avoid Them in 2025 – FDA Inspections
Definitions
| FDA | ICH E6 Guidance |
|---|---|
| All information in original records and certified copies of original records of clinical findings, observations, or other activities (in a clinical investigation) used for the reconstruction and evaluation of the trial. Source data are contained in source documents (original records or certified copies). | Original documents or data (which includes relevant metadata) or certified copies of the original documents or data, irrespective of the media used. This may include trial participants’ medical/health records/notes/charts; data provided/entered by trial participants (e.g., electronic patient-reported outcomes (ePROs)); healthcare professionals’ records from pharmacies, laboratories, and other facilities involved in the clinical trial; and data from automated instruments, such as wearables and sensors. |
What is Considered Source?
Source documentation refers to data or information captured in original records (meaning the very first place data is recorded whether electronically or on paper) and/or certified copies of original records. This includes but is not limited to:
- Informed Consent Form
- Hospital and clinic records (procedure notes, radiology reports, operative notes, discharge notes, laboratory notes, pathology notes)
- Patient interviews
- Source worksheets, checklists, patient diaries, calendars
- Patient questionnaires
- Medications flowsheets/logs
- Notes to File
- Communication records (emails, interviews, phone calls, faxes)
- Death records
What is the Purpose of Source Records?
Information captured on a source document (also known as source data and source record) serve multiple purposes: they help to reconstruct and evaluate the clinical trial, confirm the existence of participants, verify that study staff are following protocol required procedures, and ensure the integrity and accuracy of the data entered on the case report forms or electronic case report forms (eCRFs). For this discussion, we will assume most studies now utilize eCRFs.
Can an eCRF be used as the original source?
According to the FDA, data can be entered into the eCRF either manually or electronically. Data points like blood pressure, weight, temperature, pill counts, and resolution of signs and symptoms can be obtained at a study visit and can be entered directly into the eCRF by an authorized data originator (the person creating the source, including the participant). This direct entry of data can reduce errors by eliminating the transcription step before entry into the eCRF. In these instances, the eCRF is the source. If the paper transcription step is used, then the paper documentation should be retained and made available for FDA inspection. The FDA may request additional documents to corroborate a direct entry of data into the eCRF; therefore, this should be treated as the exception rather than the standard practice.
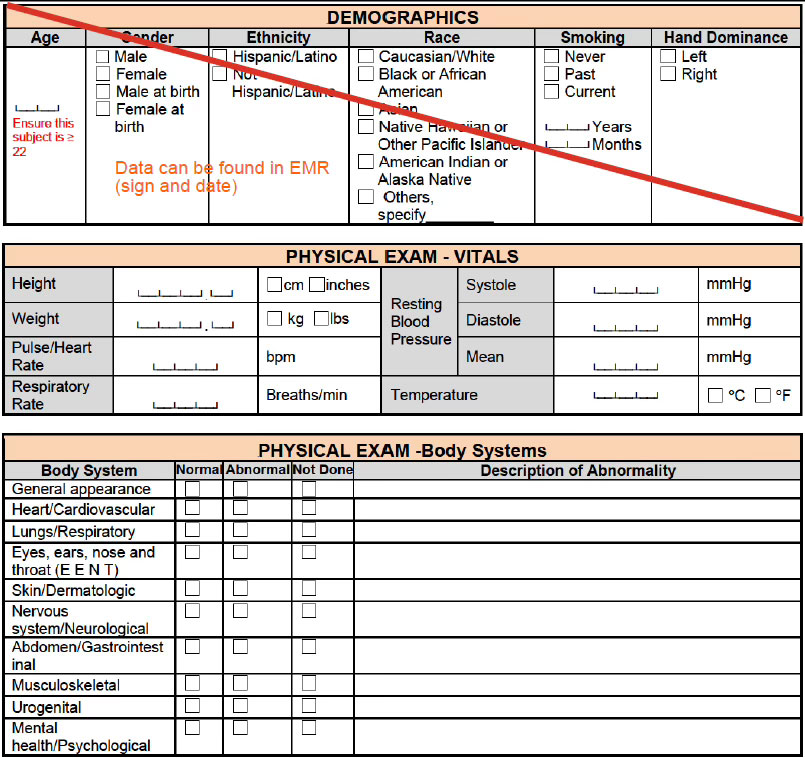
Let’s Talk Worksheets
A worksheet is often used to help collect data that is not captured elsewhere such as a visit note, the participant’s case history records or EMR; worksheets are considered source documentation. There is often debate regarding the use of worksheets, particularly when provided by the sponsor. However, worksheets are an important part of the data collection process. What are the Do’s and Don’ts when it comes to worksheets?
DOs
- Do capture data points that are not documented elsewhere or will be entered later into an eCRF.
- Do ensure participant ID, visit type, and date of record on each page.
DON’Ts
- Don’t print off eCRFs and use them as worksheets.
- Don’t capture data on a worksheet if it is already in the EMR; this introduces transcription errors and creates additional monitor burden.
How to Handle Missing Source Documentation
If a datapoint is missing in both the source and the eCRF:
- Create a query to obtain the missing data. If data is obtained, document it in the source document noting how it was obtained (e.g., telephone call to participant), and ensure it is dated and initialed by the originator.
- Determine whether this is a recurring issue that requires retraining, a CAPA, or escalation.
If a datapoint is missing in the source, but entered on the eCRF:
- In this case, the eCRF is technically the source since the data was entered there first.
- Ask the Research Coordinator (RC) where the information originated and have them add it to a source document as a “late entry” including their date and initials, as applicable.
- If documentation elsewhere confirms that the eCRF entry is the original source, no further action would be required.
- In a worst-case scenario, if there is no source located, consider removing the data as there is no documentation. Refer to your sponsor or manager for guidance.
If the datapoint is present on the source, but not entered on the eCRF:
- Verify the source is correct and create a query to have the data entered on the eCRF.
Maintaining Compliance: Practical GCP/GDP Tips
It is important not to overlook proper maintenance of source documentation. Because source documents are often living documents, the fundamentals of Good Clinical Practice (GCP) and/or Good Documentation Practice (GDP) can sometimes be forgotten – especially with new or less experienced staff. Key practices include:
- Ensure a proper audit trail: The individual who records or changes data should sign and date the entry. In some cases, having the PI sign or co-sign can demonstrate PI oversight (e.g., inclusion/exclusion criteria, adverse events, and protocol deviations).
- Correcting errors should follow GCP Guidelines:
- Draw a single line through the error (without obscuring the original entry), add the correct data, along with the initials of the person completing the change, include a reason for the correction or a note identifying where information can be found, and include the date.
- Never use white out, correction fluid, or any method that would obliterate the original entry, including write-overs.
- Never record data on scrap paper – if you do, that becomes the original source and must be secured (taped, stapled, or 3-hole punched) in the participant’s case record along with participant ID number, date of visit, and date and initials of the originator.
- Do not destroy any original records even if extensive changes require the creation of a new record.
- Never pre-date or post-date an entry or make corrections on behalf of someone else.
- Anyone signing a document should date their own signature. Do not date for someone else.
- It is acceptable to add an addendum or clarification note if needed.
Final Thoughts
Source documentation is not just a regulatory requirement—it is essential for protecting subject safety and ensuring the credibility of clinical research. By prioritizing accurate, verifiable, and traceable data, sponsors and sites can maintain compliance and uphold the integrity of their trials and ensure safeguards are in place for participant safety.
References & Footnotes
- Top 10 FDA 483 Observations of 2024 and How to Avoid Them: https://fda-news.com/top-10-fda-483-observations-of-2024-and-how-to-avoid-them/
- Electronic Source Data in Clinical Investigations: www.fda.gov/media/85183/download